


Cannabigerol: A minor phytocannabinoid with major therapeutic potential
We are learning more and more about these very unique compounds and their therapeutic applications, as well as developing synthetic derivatives that have greater potency than the parent compound.

Dr Nicole Stone | Final year PhD Student, Cannabinoid Research and Neuroscience. University of Nottingham
Over the past 30 years there have been numerous scientific breakthroughs in a bid to unlock the full potential of cannabis sativa. One of the most abundant compounds found in cannabis, cannabidiol (CBD), has been hailed as a wonder drug with infinite medicinal properties. As CBD does not produce euphoric effects (i.e gives you a high) it is considered to be a more desirable drug candidate than tetrahydrocannabinol (Δ9-THC) in the clinical setting. CBD is currently licensed as a treatment for rare forms of childhood epilepsy and is in clinical trials for several conditions including anxiety, fibromyalgia, post-traumatic stress disorder and pain. Moreover, the recent surge in over-the-counter supplements and healthcare products containing CBD has led to patients self-medicating for conditions such as anxiety, pain and even skin disorders such as acne and psoriasis. So, two major questions currently being asked by researchers are:
What are the properties of other compounds present in cannabis?
Could these compounds have medicinal benefit?
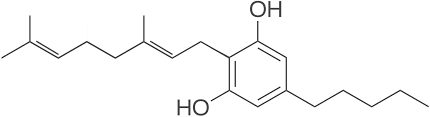
There are over 120 different compounds that have been identified and isolated from the cannabis plant, however compared to Δ9-THC and CBD they have received significantly less scientific investigation. These compounds are referred to as the ‘minor phytocannabinoids’ and limited data has shown they have interesting pharmacological properties. Cannabigerol (CBG) was first isolated in 1964, by the same group that identified and reported the structure of Δ9-THC, the chemical in cannabis that produces euphoric effects. Like other cannabinoids, CBG exhibits anti-inflammatory, neuroprotective and anti-cancer properties and some outlets have hailed CBG as ‘the new and improved CBD’. Whilst there is preliminary evidence to suggest that CBG is protective in preclinical models, there is still a great deal we do not know about the pharmacology of CBG and not enough data to confirm therapeutic translatability in humans-at least not yet.
According to the World Health Organisation (WHO) neurodegenerative disorders are predicted to become the second most prevalent cause of death by 2040. Multiple failures of drugs developed to treat neurological and neurodegenerative conditions stems from the fact these diseases are highly complex and multifactorial. Numerous studies have shown cannabinoids exhibit neuroprotective properties, thought to be in part due to their unique polypharmacology (the ability of a drug to bind to multiple pharmacological targets) and potent anti-inflammatory and antioxidant effects. CBG has been shown to be neuroprotective in pre-clinical models of Huntington’s disease, Parkinson’s disease and amyotrophic lateral sclerosis (ALS) and researchers have identified that CBG displays significant anti-inflammatory effects that were particularly effective in dampening microglial activation. Microglia are resident brain immune cells, where they have a dustbin-like function helping clear debris and unwanted substances which are harmful to neuronal health. In conditions such as Huntington’s, Parkinson’s and ALS these cells become dysfunctional and promote inflammation, which is harmful to the brain and contributes to disease progression. Given that CBG is anti-inflammatory, it may offer a unique therapeutic strategy against microglial dysfunction and help prevent inflammation in the brain which contributes to neuronal cell death in these disorders. A recent study also reported the efficacy of CBG in a cellular model of glioblastoma, an aggressive form of brain cancer. This study found that CBG alone and in combination with CBD displayed significant antitumour effects. These early data are incredibly exciting and altogether warrant further investigation into CBG and its neuroprotective effects.
Inflammatory bowel disease (IBD) is a global problem, and the incidence of this debilitating condition is on the rise, particularly in newly industrialised counties. Similarly, colorectal cancer is the 3rd most common cancer in the UK with 1 in 19 people predicted to develop colorectal cancer in their lifetime. In addition to its neuroprotective properties, CBG has shown efficacy in pre-clinical models of inflammatory bowel disease (IBD) and colorectal cancer. In IBD, researchers found CBG reduced inflammation in the colon and improved overall tissue recovery whilst models of colorectal cancer found that CBG treatment reduced tumour growth. These data suggest that CBG may be pursued clinically either alone or as an adjuvant therapy, however this remains to be explored.

Interestingly, research groups have developed quinone derivatives of CBG (known as VCE-003 and VCE-003.2) which are formed by the oxidation of the parent molecule. These compounds display increased affinity for a known cannabinoid target, peroxisome proliferator-activated receptor gamma (PPARγ), which governs many physiological responses, including lipid (fat) metabolism. PPARγ is of interest to researchers because its activation has anti-inflammatory effects. Interestingly, Emerald Health Pharmaceuticals has orphan designation granted in the US for VCE-003.2 to treat Parkinson’s and Huntington’s disease, which is currently in the formulation phase, and it will be interesting to follow the progress of this compound through preclinical development and possibly into clinical trial.
Research into CBG and other minor phytocannabinoids is rapidly progressing but the majority of studies are still very much preliminary stage. We are learning more and more about these very unique compounds and their therapeutic applications, as well as developing synthetic derivatives that have greater potency than the parent compound. CBG clearly has therapeutic potential, however we still need fully understand its pharmacological profile and test this compound in more clinically translatable models. Collaborations with pharmaceutical companies, innovative technologies and novel modelling capabilities, together with advice from specialist clinicians and scientists will help develop the knowledge we have on these minor phytocannabinoids and optimise their progression into the clinic.
Really nicely written! Very informative